“Men are silent stoics; women hysterical hypochondriacs,” writes The Guardian.
In the past, the diagnosis of “hysteria” was a catch-all term for complaints of discomfort reported mainly by women—including anxiety and irritability—making the term both convenient and dangerous. Only in 1980 was was “hysterical neurosis” removed from psychology textbooks, and yet its legacy lives on; studies show that female patients complain about higher levels of pain more frequently but are taken less seriously by medical professionals. One study concluded that a primary factor for the imbalance in treatment was gender bias—specifically, “A long history within our culture of regarding women’s reasoning capacity as limited.”
Feminist author Maya Dusenbery calls this the “trust gap,” where women are more likely to be disregarded in healthcare and treatment than men are.
In a Q&A session with the Greater Good Magazine at UC Berkeley, after reading anecdotes from women seeking diagnoses, Dusenbery said, “There was an implication that their physical symptoms were all in their heads, and they were being offered antidepressants or told they were ‘making their symptoms up’ to get attention.”
This is especially the case for women of color. Above all, Black women are a target of discrimination within the healthcare system, even when socioeconomic factors are controlled. Research shows that Black women are less likely to be prescribed pain medication by emergency room physicians despite experiencing the equivalent levels of pain and symptoms to white women and three times more likely to die in childbirth.
There was an implication that their physical symptoms were all in their heads, and they were being offered antidepressants or told they were ‘making their symptoms up’ to get attention.
The obstruction of medical diagnoses is just one of the many effects of gender bias in treating women. Endometriosis, a chronic illness that causes debilitating uterine pain during menstruation, is estimated to affect at least one in ten women but takes an average of 7.5 years to diagnose. This means that at least 10% of women have to live with chronic monthly pain for three-quarters of a decade before being able to receive treatment. Another 2017 study found that women had to wait longer than men to receive their diagnosis after first recognizing cancer symptoms and concluded that it could take a woman up to 31 days more than a man to receive a diagnosis. Other studies show that women were less likely to receive pain medication in the ER and, when experiencing a heart attack, seven times more likely to be misdiagnosed and sent home.
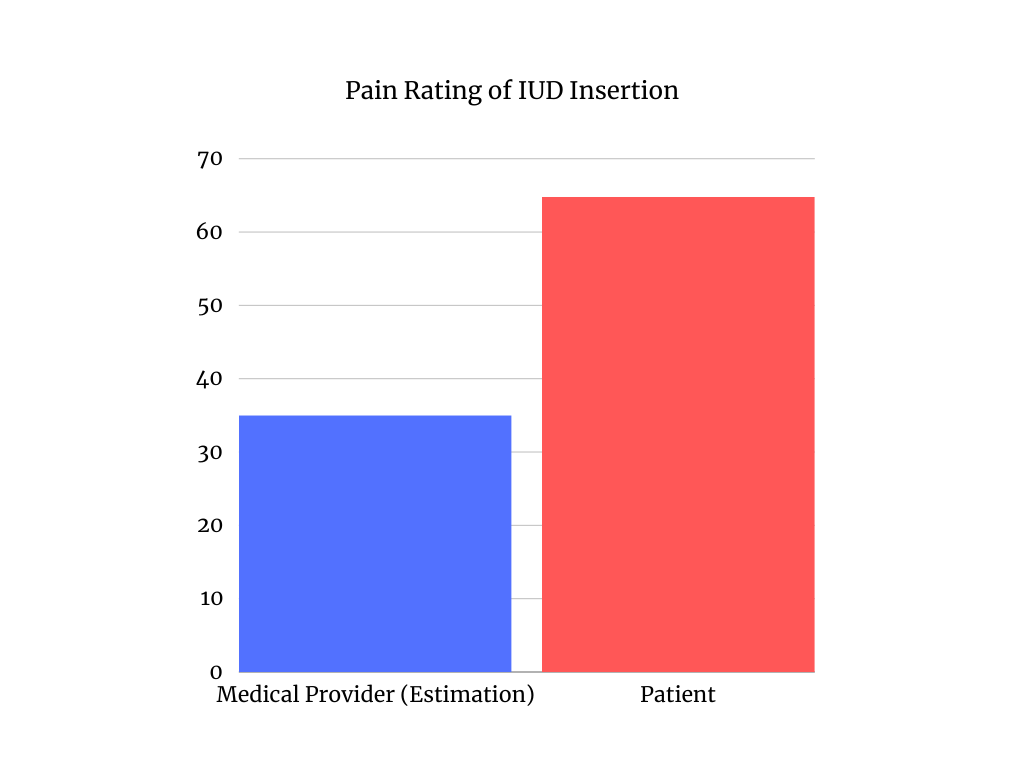
When women are getting intrauterine devices (IUD), a form of birth control, they are told to take the same medication that one would take for a headache. According to a 2013 study, medical providers estimated the pain to be around 35 on a scale of 100; patients rated the pain as 64.8 on average.
An anonymous student shared her experience getting an IUD insertion. She said, “I definitely had a good experience with the doctors, but when I asked them if they would give me anything for the procedure, they told me I could pop an Advil or a Tylenol. I know people who have had extremely painful insertions, and it feels absurd that they won’t offer anything.”
She added, “There are so many different forms of birth control, which is great, but then you have to deal with finding the ones that work for you when men could just get a vasectomy that they are fully under anesthesia for or wear a piece of rubber.”
Women today enter a healthcare system that is much more accommodating than in the past, though the information they are given still doesn’t adequately prepare them for their endeavors.
A second anonymous student was on four different birth controls before finding one that fit her, a surprisingly difficult and unclear process. She said, “I tried the Nexplanon implant because they said it was less hormonal and had few side effects. But, I was super fatigued—which they later told me was another possible side effect. For a month straight, I would have to come home from school every day because I was so tired I needed to take a nap for half the day.”
In addition, when they removed the implant, she explained, “It was one of the most painful experiences in my life. They told me it would be easy because they just had to push it out, but they were digging in my arm for so long because it was surprisingly difficult for them to find.”
She added, “I felt supported, but they did not give enough information to me and my parents, which made us really upset because of all the painful things that happened.”
To better accommodate this imperfect system, it’s essential to trust your own body and advocate for yourself. Additionally, Psychology Today advised, “Finding a supportive person can be as simple as asking a friend, sister, or daughter to come to an appointment with you, take notes, and ask questions. If you’re not comfortable starting a conversation, they might [start] it, or give you moral support.”
I felt supported, but they did not give enough information to me and my parents, which made us really upset because of all the painful things that happened.
The final piece of advice is to simply find a new doctor if you feel you aren’t having your concerns recognized. In the New York Times, Dr. Elizabeth Comen acknowledged, “This can be easier said than done […] but a trusting and respectful relationship with your healthcare provider is every patient’s right.”
Advocating for yourself can be difficult, especially when you are in such a vulnerable position. But one of the anonymous students said, “I definitely think it’s always worth advocating for yourself, and I’m very glad I asked.”